
What Causes Menopause? And Why It’s Not Just About Running Out of Eggs 😉

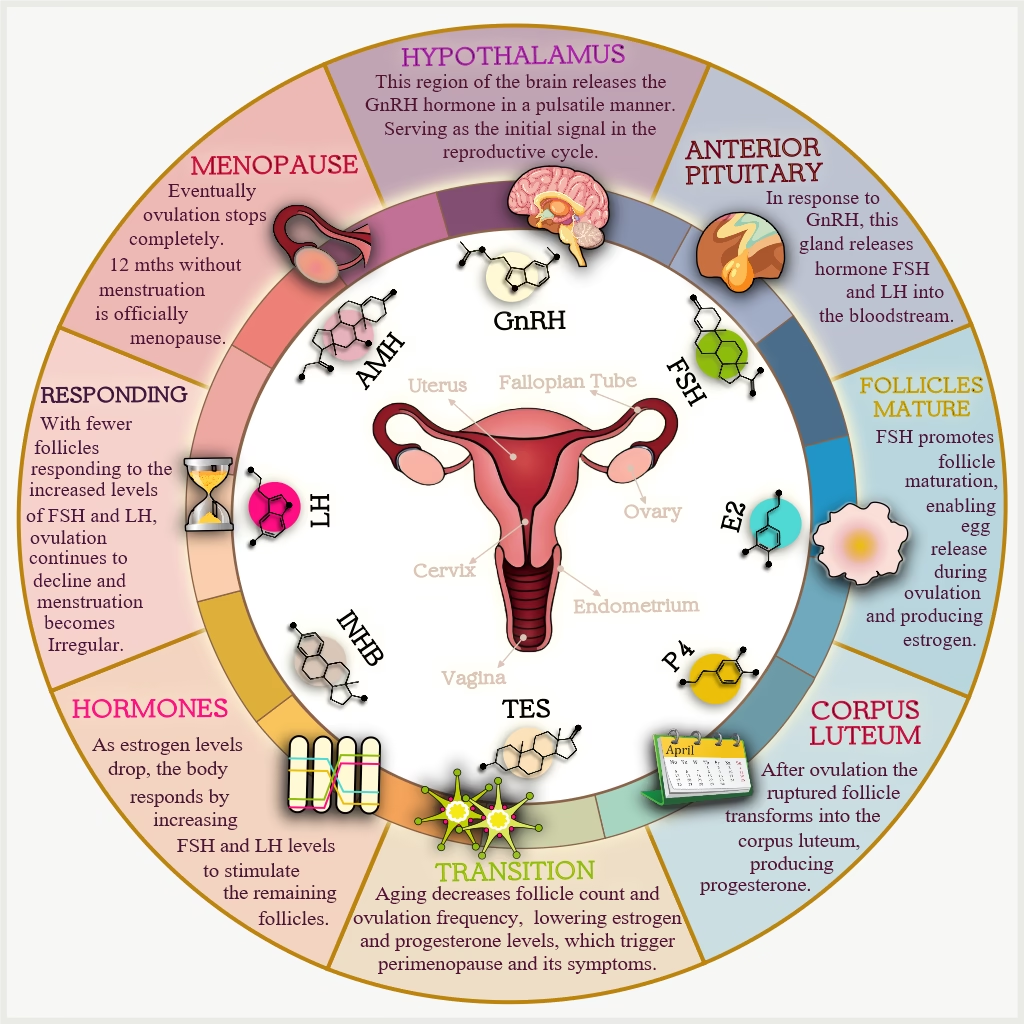
This diagram shows how hormones regulate the menstrual cycle.
Your Brain’s Command Center: The Hypothalamus Takes Charge
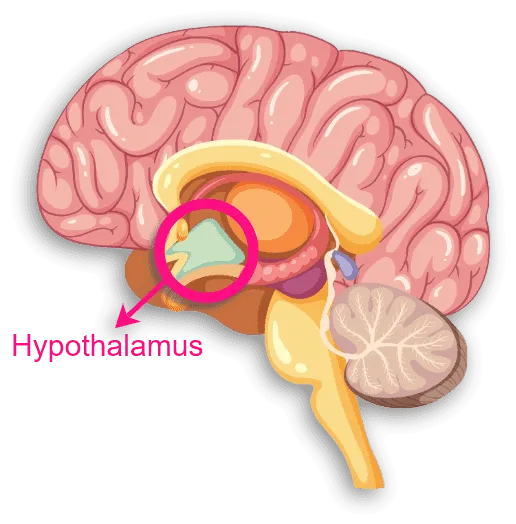
Deep in your brain sits a tiny region called the hypothalamus. However, don’t let its size fool you – this little powerhouse is basically mission control for your entire reproductive system. It’s the boss, the director, the one calling all the shots.
The hypothalamus produces a hormone called GnRH. That stands for Gonadotropin-Releasing Hormone, but let’s stick with the abbreviation. Life’s too short, darling. Meanwhile, GnRH is like that manager who sends out carefully timed emails throughout the day to keep everyone on task. It doesn’t flood your inbox all at once, instead, it releases in rhythmic pulses, little bursts of “Time to get to work!” signals.
These pulses travel down to your pituitary gland. This is another small but mighty player in your brain. They tell it to release two crucial hormones: FSH (Follicle-Stimulating Hormone) and LH (Luteinizing Hormone). How much FSH and LH get released? That depends on the frequency and intensity of these GnRH pulses. It’s a beautifully choreographed system when everything’s working smoothly.
Therefore, think of it as your body’s internal email chain. The hypothalamus sends the memo. The pituitary gland reads it and takes action. Your ovaries receive the assignment. Everyone knows their role, everyone hits their marks, and the show goes on month after month, year after year.
10 Perimenopause Surprises
Welcome to perimenopause, darling. The biological surprise party where all the guests show up unannounced, nobody brought wine, and the host (that's you) is standing there thinking, "I'm 42. This wasn't supposed to start yet.
This guide tells you what no one else will tell you. Not even your doctor.
The Anterior Pituitary Gland: Your Hormone Dispatch Center
Once your pituitary gland receives those GnRH pulses, it springs into action. As a result, it releases FSH and LH into your bloodstream. These hormones travel down to your ovaries like messengers carrying important instructions.
Here’s where it gets fascinating, darling. Because remember those eggs I mentioned? The ones you were born with? They’re not just sitting around waiting. Each egg is housed in a tiny structure called a follicle. Your ovaries contain hundreds of thousands of these immature follicles, and every month, FSH’s job is to wake up a batch of them and say, “Ladies, it’s audition time!”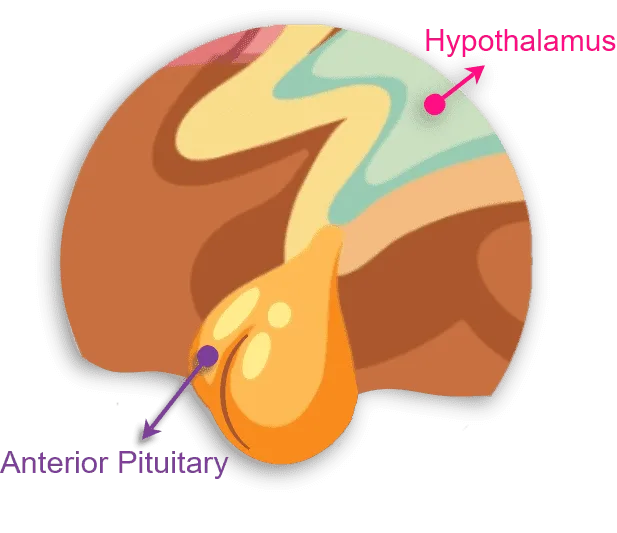
FSH shows up and stimulates multiple follicles to start maturing. It’s like the first round of auditions for a lead role, lots of hopefuls, but only one will make it to opening night.
As these follicles mature, they produce hormones themselves. This includes estrogen (the star of the show) and supporting players Anti-Müllerian Hormone (AMH) and Inhibin-B.
AMH acts as quality control, making sure not too many follicles mature at once. Inhibin-B provides feedback to your pituitary gland, essentially saying, “We’ve got enough FSH for now, thanks!” It’s a sophisticated feedback loop that keeps everything balanced.
Meanwhile, LH joins the party mid-cycle with a dramatic surge. When estrogen levels rise high enough (produced by those maturing follicles), they trigger a massive spike in LH. This LH surge is the signal for the dominant follicle, the one that won the audition, to release its egg. That’s ovulation, honey. The main event.
Follicle Maturing and Estrogen Production
As follicles mature, they start producing estrogen. Now, estrogen isn’t just sitting around looking pretty – this hormone is working harder than you did in your twenties, juggling multiple jobs simultaneously:
 |
It regulates your menstrual cycle by thickening the endometrium (your uterine lining, if you want to get technical about it). Think of it as interior decorating for potential pregnancy – fresh linens, plumped pillows, the works. |
 |
It also acts as your body’s quality control manager, constantly sending feedback to your hypothalamus and pituitary gland about GnRH, FSH, and LH levels. Too much? Too little? Estrogen’s on it, adjusting the dials to keep everything humming along smoothly. |
 |
Each cycle, estrogen helps select the healthiest follicle to mature and ovulate. It’s essentially casting director for your monthly egg release, choosing the star performer from dozens of hopefuls. |
 |
And here’s something they rarely mention: estrogen maintains your bone density. It reduces osteoclast activity (cells that break down bone) while increasing osteoblast activity (cells that build bone). Translation? Estrogen’s been quietly protecting your skeleton from osteoporosis this entire time. |
|
It regulates your menstrual cycle by thickening the endometrium (your uterine lining, if you want to get technical about it). Think of it as interior decorating for potential pregnancy – fresh linens, plumped pillows, the works. |
|
It also acts as your body’s quality control manager, constantly sending feedback to your hypothalamus and pituitary gland about GnRH, FSH, and LH levels. Too much? Too little? Estrogen’s on it, adjusting the dials to keep everything humming along smoothly. |
|
Each cycle, estrogen helps select the healthiest follicle to mature and ovulate. It’s essentially casting director for your monthly egg release, choosing the star performer from dozens of hopefuls. |
|
And here’s something they rarely mention: estrogen maintains your bone density. It reduces osteoclast activity (cells that break down bone) while increasing osteoblast activity (cells that build bone). Translation? Estrogen’s been quietly protecting your skeleton from osteoporosis this entire time. |
Ovulation and the Corpus Luteum
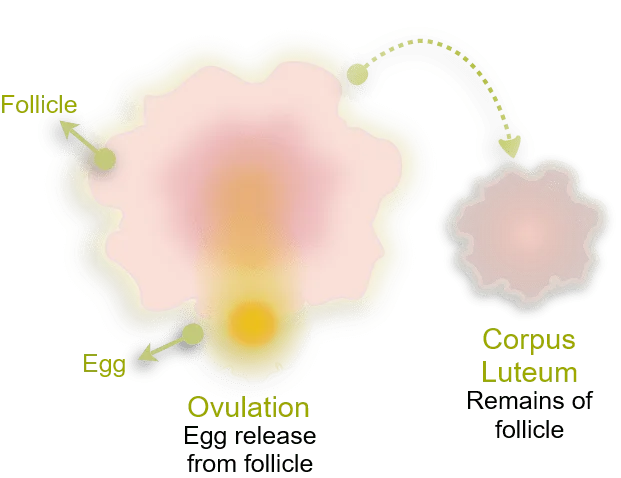
Ovulation is the moment when your dominant follicle ruptures. As a result, it releases a mature egg into your fallopian tube. It’s the climax of your menstrual cycle, the reason all this hormonal coordination exists in the first place.
However, the story doesn’t end there. After the egg is released, that ruptured follicle doesn’t just disappear. Instead, it transforms into something called the corpus luteumm a temporary hormone-producing structure that’s absolutely crucial for what comes next.
The corpus luteum produces progesterone (and some estrogen). Therefore, it prepares your uterine lining for a potential pregnancy. It’s like fluffing the pillows and putting fresh sheets on the bed for an important guest. If a fertilized egg arrives and implants, the corpus luteum gets the signal. As a result, it keeps producing progesterone to support the early pregnancy.
However, and this is the case most months, pregnancy doesn’t occur. Therefore, the corpus luteum breaks down after about two weeks. Consequently, progesterone and estrogen levels drop, your uterine lining sheds (hello, period), and the whole cycle starts again. The corpus luteum degenerates into scar tissue called the corpus albicans, which your ovary eventually absorbs. Clean slate. New month. Fresh start.
This entire process repeats itself month after month, year after year, for decades. GnRH pulses trigger follicle maturation. Follicle maturation leads to ovulation. Ovulation creates the corpus luteum. It’s been your body’s routine since puberty, as reliable as your morning coffee ritual. Until it isn’t.
What Causes Menopause? The Transition Begins
Here’s where things get interesting, darling. Because menopause isn’t an overnight event, it’s a gradual transition that can take years. Moreover, it all comes down to one simple, unavoidable fact: you’re running out of eggs.
Remember that collection of 500,000 to one million follicles you were born with? Well, you’ve been using them up, not just during ovulation, but also through a process called follicular atresia, where follicles naturally deteriorate even when they’re not selected for ovulation. By the time you hit your late 30s or early 40s, therefore, your ovarian reserve has significantly diminished.
As you approach your late 40s or early 50s (though everyone’s timeline is different, naturally), you enter perimenopause. This is the transition phase. Some call it the Early Menopause Transition. This is Stage -2 in the STRAW+10 system. I call it the “What the hell is happening to my body?” phase.
Menopause Transition
(click to enlarge image)

This diagram shows how hormones drive changes during the menopause transition.
The Follicle Shortage: When Supply Can’t Meet Demande
The defining feature of perimenopause? Your ovaries are running low on responsive follicles. However, you still have some, but not nearly as many as you used to, and the ones remaining are
getting less enthusiastic about responding to hormonal signals.
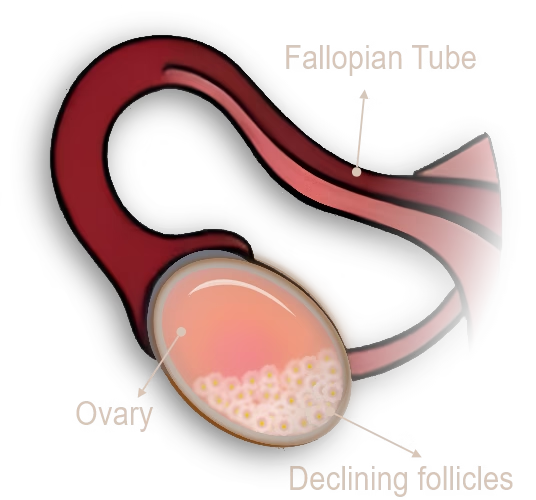
For instance, it’s like having a theater company where most of the actors have retired. You’re still trying to put on shows, but you’re working with a skeleton crew, and they’re not as spry as they used to be.
Your body, however, doesn’t immediately realize the pool is running dry. So what does it do? It tries harder.
FSH and LH Go Into Overdrive: The Panic Mode
As your estrogen levels start to decline (because fewer follicles are maturing and producing estrogen), your pituitary gland notices. “Wait,” it thinks, “estrogen is dropping! We need more follicles to mature! Send more FSH! Send more LH!”
Therefore, your body cranks up FSH and LH production. It floods your system with these hormones in an attempt to stimulate your remaining follicles. It’s like turning up the volume on a speaker, hoping that will make the music better. Spoiler alert: it doesn’t.
In fact, this prolonged exposure to high levels of FSH and LH actually makes things worse. The follicles become desensitized to these hormones – like developing immunity to your alarm clock after hitting snooze too many times. They become less and less responsive, less able to mature properly, less likely to ovulate.
This is when your menstrual cycle starts getting weird, darling. Because with fewer follicles responding, you might skip ovulation some months. Without ovulation, no corpus luteum forms. As a result, progesterone levels drop. Without proper progesterone, your cycle becomes irregular.
Some months your period arrives early. Other months it’s late. Meanwhile, sometimes it’s heavy, flooding like you’re a teenager again. Other times it’s barely there, just a whisper of what it used to be. You might skip a month entirely, think “Is this it? Am I done?” and then boom, Aunt Flo crashes back into your life like an uninvited dinner guest.
Welcome to perimenopause, where predictability goes out the window and your body writes its own chaotic schedule.
The Declining Response: When the Curtain Starts to Fall
As fewer and fewer follicles respond to those elevated FSH and LH levels, ovulation becomes increasingly sporadic. Consequently, the corpus luteum forms less frequently, which means progesterone production drops even further. Your cycle, once a reliable monthly visitor, becomes as unpredictable as a cat’s affection.
This decline isn’t sudden, it gradual, happening over years. Your body is slowly winding down the reproductive machinery, like a factory gradually reducing production before closing its doors entirely.
The Symptoms: What You Experience as Menopause Begins
During this time, you might experience all sorts of delightful symptoms. Hot flashes that arrive without warning, turning you into a human radiator. Night sweats that drench your sheets and disrupt your sleep. Mood swings that have you crying at commercials and snapping at loved ones over minor annoyances. Brain fog that makes you forget why you walked into a room or where you left your keys (again).
These symptoms aren’t in your head, honey. Instead, they’re the direct result of your fluctuating hormone levels. Your body is adjusting to this new hormonal landscape, and it’s not always a smooth transition.
Summarising What Causes Menopause
Eventually, after months or years of this perimenopausal chaos, your ovaries effectively stop releasing eggs altogether. As a result, the follicles are depleted, exhausted, done. Without ovulation, no corpus luteum forms. Without a corpus luteum, estrogen and progesterone levels drop to their lowest levels yet and stay there.
When you’ve gone 12 consecutive months without a menstrual period, you’ve officially reached menopause. Therefore, mark that date in your calendar, darling, it’s your reproductive retirement party! This is Stage +1 of the STRAW+10 system, or Early Postmenopause.
At this point, your hormone levels have fundamentally shifted. Meanwhile, estrogen and progesterone are low and staying low. FSH and LH remain elevated, your pituitary gland is still shouting “Make more eggs!” even though your ovaries have hung up the “Closed” sign and gone home.
This new hormonal reality defines postmenopause. Specifically: low estrogen, low progesterone, high FSH, high LH. And it comes with its own set of challenges.
Low estrogen affects more than just your reproductive system, sweetie. In fact, it impacts your bones (increasing osteoporosis risk), your cardiovascular system (affecting heart health), your skin (hello, dryness and loss of elasticity), your vaginal tissues (leading to dryness and discomfort), and even your mood and cognitive function. Estrogen has been your body’s multitasking superstar for decades, and its absence is felt throughout multiple systems.
However, here’s the thing, while the symptoms can be challenging, they’re not insurmountable. Understanding what’s happening and why empowers you to manage them effectively and embrace this new chapter.
How Hormonal Changes Cause Menopause
(click to enlarge image)
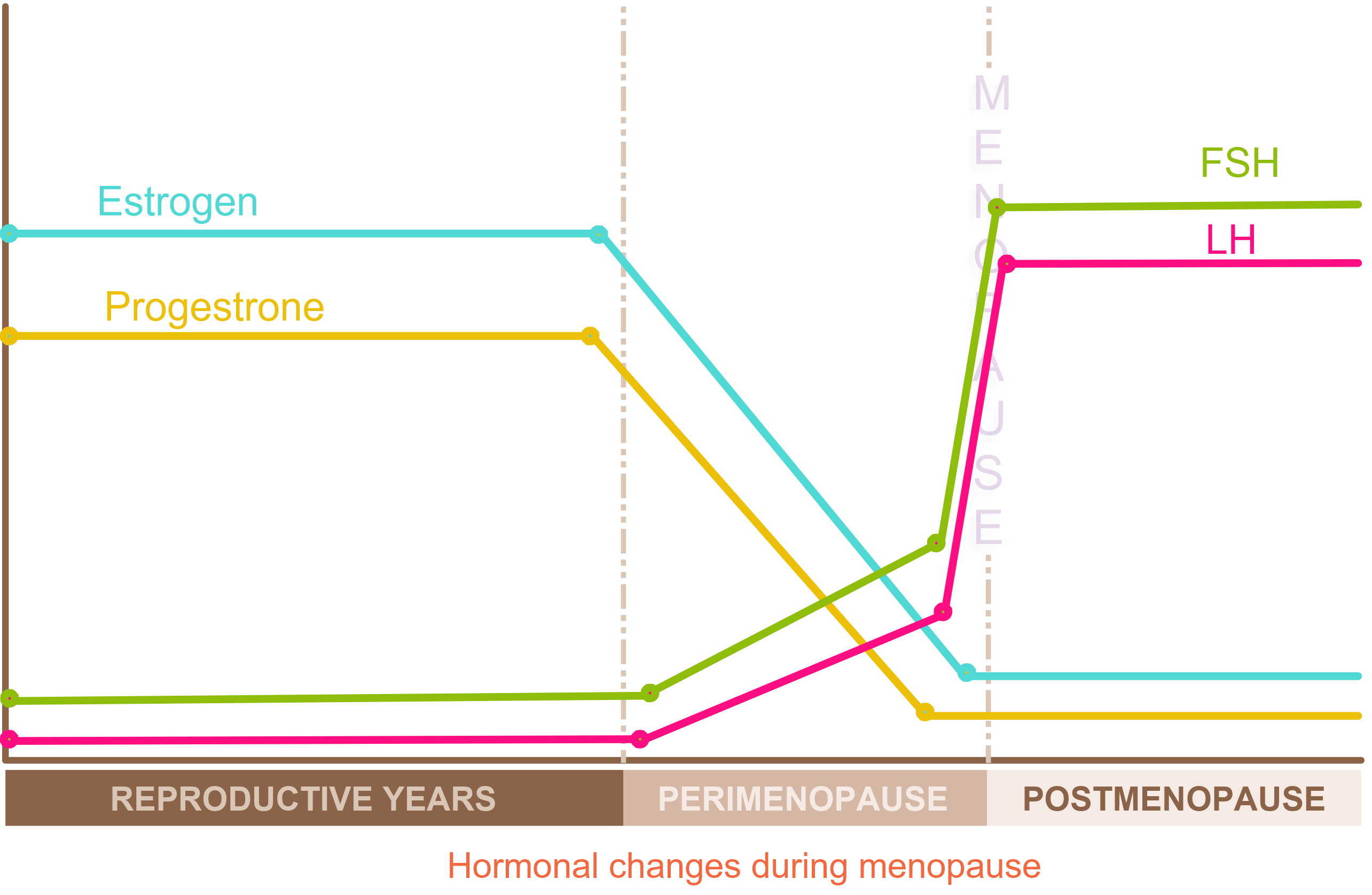
Menopause is characterised by low levels of estrogen and progesterone, alongside elevated levels of FSH and LH. The decline in estrogen can lead to a range of symptoms, including hot flashes, night sweats, mood swings, and vaginal dryness.
The Beautiful Truth About This Transition
Here’s what they don’t always tell you about menopause, darling: it’s not just an ending. In fact, your reproductive years are concluding, but a whole new chapter is beginning.
No more periods means no more monthly disruptions. Therefore, no more cramping. No more worrying about contraception or unexpected pregnancies. No more PMS mood swings or buying tampons in bulk. There’s genuine freedom in that.
Moreover, many women report feeling more confident, more self-assured, and more willing to speak their minds in their post-menopausal years. Whether that’s due to hormonal changes, life experience, or simply giving fewer damns about what others think is up for debate. However, the result? A sense of liberation that’s absolutely worth celebrating.
So yes, menopause is caused by aging and the natural depletion of your ovarian reserve. However, what it represents, freedom, wisdom, and a new phase of life lived on your terms, is something far more valuable than a simple biological explanation can capture.
Welcome to the next chapter, honey. It’s going to be fabulous. 💋


Leave a Comment