

Menopause Hormones: The Royal Ballet
Menopause Hormones: The Royal Ballet
Picture this, sweetheart: menopause hormones are like Fred Astaire and Ginger Rogers, executing a perfectly choreographed dance number in your fabulous body.
But here’s the plot twist, as we age, our Fred starts stepping on Ginger’s toes, and suddenly the whole performance goes delightfully off-script.
Welcome to the grand finale of your reproductive years, where the curtain call is anything but predictable!
Let’s pull back the velvet curtain and meet the star performers in this hormonal ballet. Trust me, honey, once you know who’s who, the whole show makes a lot more sense.
Meet Your Cast of Key Characters

GnRH: The Diva Director
If your reproductive system were a Broadway production, GnRH would be the director. She’d have the megaphone, the clipboard, and probably a very expensive latte. This little hormone bosses around FSH and LH like they’re backup dancers. She orchestrates the entire menstrual cycle from its perky opening number right through to menopause’s dramatic finale.
What Exactly Is This GnRH Character?
Gonadotropin Releasing Hormone (or GnRH, because who has time for that mouthful?) is your body’s ultimate stage manager. It lives rent-free in a cozy little spot in your brain called the hypothalamus. Think of it as the control room where all the reproductive magic happens. This clever little hormone sets the tempo for your entire reproductive cycle, making it absolutely essential when we’re chatting about menopause hormones.
What’s GnRH’s day job? Regulating your reproductive system by telling two other hormone hotshots, follicle-stimulating hormone (FSH) and luteinizing hormone (LH), when to make their entrance from the pituitary gland. These two are absolutely critical for keeping your ovaries happy and functional.
GnRH’s Role in Baby-Making Business
GnRH is like that friend who sends you texts in short, rhythmic bursts instead of one long essay. Bless them. It fires off from the hypothalamus in these adorable little pulses, and honey, that rhythm is everything.
These pulses keep the pituitary gland’s receptors on their toes. They prevent the receptors from getting bored and tuning out, which would happen faster than you can say “hormone resistance” if GnRH showed up constantly.

These perfectly timed pulses tell the pituitary gland when to release FSH and LH. The frequency and intensity of these GnRH pulses can favor one hormone over the other. It’s like a conductor emphasizing the violins over the cellos.
FSH gets the follicles (those little egg containers) ready for their debut. Meanwhile, LH is the one yelling “Action!” when it’s time for ovulation, the grand release of a mature egg from your ovary.
So GnRH is basically coordinating this entire production. It makes sure your menstrual cycle flows smoother than a silk nightgown.
By controlling FSH and LH, it’s also pulling the strings on estrogen and progesterone production, those vital hormones that maintain your uterine lining and prep your body for a possible pregnancy (whether you’re auditioning for that role or not).
10 Perimenopause Surprises
Welcome to perimenopause, darling. The biological surprise party where all the guests show up unannounced, nobody brought wine, and the host (that's you) is standing there thinking, "I'm 42. This wasn't supposed to start yet.
This guide tells you what no one else will tell you. Not even your doctor.
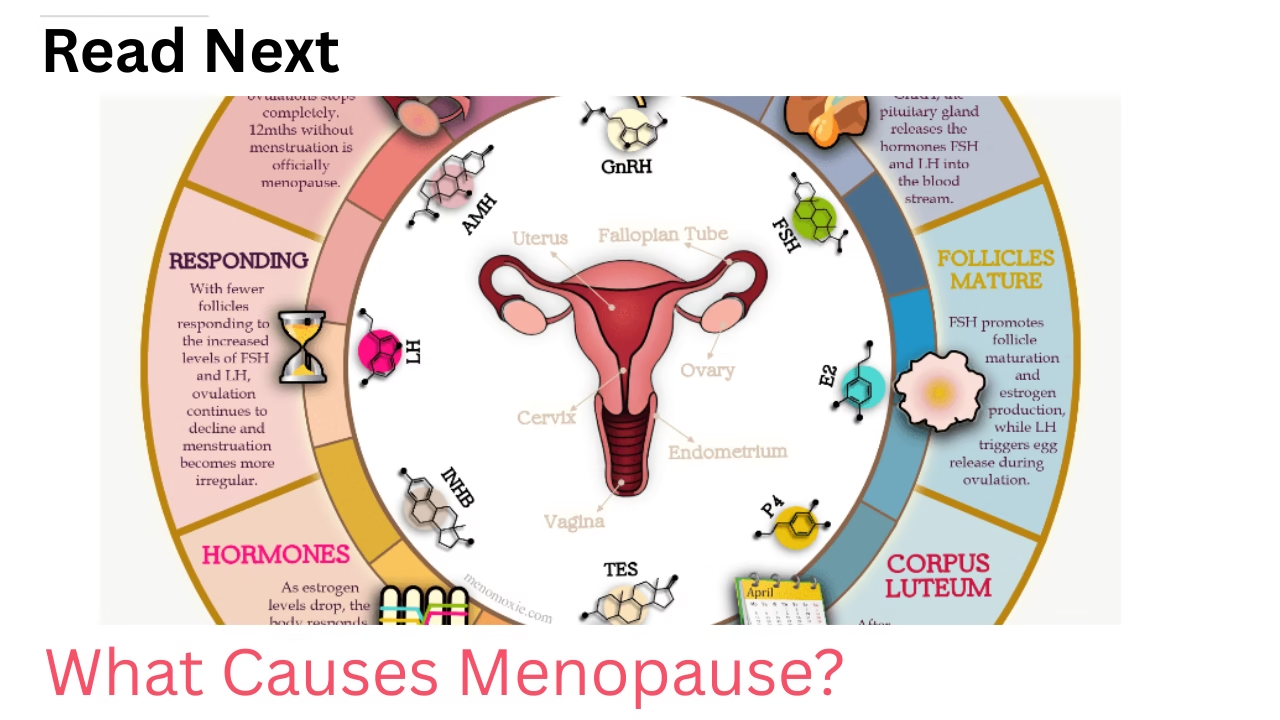
When GnRH Goes Rogue During Menopause
Now here’s where things get interesting, darling. As we mature like fine wine (or aged cheddar, depending on the day), our ovaries start phoning it in. They slow down their production of estrogen and progesterone. They’ve decided retirement sounds pretty good, actually.
This gradual ovarian slow-down is the fundamental biological process that ultimately leads to menopause.
But GnRH? Oh honey, GnRH doesn’t get the memo. Instead, it panics like a stage manager whose lead actors just called in sick.
The hypothalamus cranks up GnRH production, which then floods the pituitary gland with “Make MORE FSH and LH!” messages. It’s trying desperately to wake up those sleepy follicles and get ovulation back on track.
Here’s the kicker: those increased levels of FSH and LH start overstimulating the remaining follicles. It’s like an overenthusiastic personal trainer. And just like when someone pushes you too hard at the gym, these follicles become less responsive to the very hormones trying to motivate them.
They’re basically saying, “Back off, we’re tired!” This creates a vicious cycle where estrogen and progesterone levels keep dropping despite everyone’s best efforts.
This hormonal tug-of-war marks your official transition into menopause. It showcases the complicated relationship between your endocrine system and your aging reproductive organs. It’s like watching a soap opera unfold inside your own body!
That transition isn’t a single moment, but a series of clearly defined stages — each with its own hormonal patterns.
The Fallout from GnRH’s Midlife Crisis
Those sky-high levels of GnRH, FSH, and LH, all caused by your ovarian follicles taking an early retirement, create a hormonal imbalance. It’s about as balanced as a seesaw with an elephant on one side.
This is what triggers those delightful menopausal calling cards: hot flashes that could melt an ice sculpture, night sweats that turn your bed into a water park, and periods so irregular they make your teenage cycle look predictable.
These symptoms don’t show up the same way for everyone — they tend to shift depending on which stage of the transition you’re in.
Can We Test for GnRH to Diagnose Menopause?

Well, sweetie, here’s the thing: measuring GnRH directly is about as practical as trying to catch fireflies in a hurricane. It pulses in tiny bursts, making it harder to pin down than your car keys on a Monday morning.
So instead, doctors take the smart route. They measure FSH and LH levels in your blood, they’re much easier to detect and tell us everything we need to know about what GnRH is up to behind the scenes.
FSH: The Overzealous Stage Manager

What’s FSH All About?
Follicle-stimulating hormone (FSH for those of us who can’t be bothered with syllables) comes courtesy of your pituitary gland.
That’s the tiny but mighty powerhouse at the base of your brain. Its main gig? Getting those follicles (the cute little sacs housing your developing eggs) ready for their big debut.
FSH is absolutely crucial when we’re discussing menopause hormones, honey. It’s part of this incredibly intricate communication network called the hypothalamic-pituitary-ovarian axis (or HPO axis, because scientists love their acronyms almost as much as we love our excuses for opening a bottle).
Through this system, FSH teams up with LH, they’re basically the dynamic duo of your menstrual cycle.
When it comes to understanding the relationship between menopause hormones, FSH is like that friend who can’t keep a secret. Its levels tell your doctor everything they need to know about where you are on this reproductive journey.
If you’re wondering where you might be right now, the Perimenopause Quiz can help you get your bearings using real patterns, not guesswork.
FSH’s Day Job in Baby-Making

At the start of each menstrual cycle, FSH levels rise like the curtain on opening night. They signal your ovaries to start prepping a group of follicles for their moment in the spotlight.
Usually, one follicle becomes the star of the show (the “dominant” one, if you want to get technical). Meanwhile, the others gracefully bow out and regress.
But wait, there’s more! FSH also tells those growing follicles to pump out estrogen. This estrogen boost is essential for getting your uterus ready for a potential pregnancy.
It also triggers all sorts of other hormonal changes throughout your body. It’s like the domino effect, but with more mood swings.
When FSH Goes Into Overdrive During Menopause
Here’s where things get spicy, sweetheart. FSH levels start creeping up about six years before menopause. Talk about advance notice!
Then, in the two years leading up to your final period (your period’s farewell tour, if you will), FSH levels shoot up faster than your hand reaching for the wine bottle after a long day. About two years after menopause, these levels finally settle down and stabilize.
The combination of skyrocketing FSH and LH levels, paired with plummeting estrogen and progesterone (plus a whole cocktail of other hormonal shenanigans), creates the perfect storm. This is where those delightful menopausal symptoms we all know and love come from.
What You Might Experience:
Irregular periods: Your menstrual cycle becomes about as predictable as British weather. As ovarian function declines and hormones fluctuate like a teenager’s mood, your periods start showing up whenever they please.
Hot flashes and night sweats: These little gems are primarily thanks to your estrogen levels doing the limbo. How low can they go? They’re the calling cards of menopause, arriving uninvited and overstaying their welcome.
Mood changes: When estrogen, progesterone, and their hormone friends start fluctuating, they mess with your neurotransmitters. This affects your mood and emotional well-being. It’s like having an emotional weather system inside your body. And honey, sometimes it’s stormy.
Vaginal dryness: As estrogen levels decline, your vaginal tissues decide lubrication is overrated. Spoiler alert: it’s not.
Now, here’s the thing, darling, while rising FSH levels are a telltale sign you’re entering the menopausal transition, most of these symptoms are actually more directly linked to declining estrogen.
FSH is just the messenger. Estrogen is the one really calling the shots (or rather, NOT calling them anymore).
The timing and severity of these symptoms vary wildly between women. Some sail through menopause like it’s a Mediterranean cruise. Others feel like they’re navigating a hurricane in a dinghy. There’s no one-size-fits-all experience here, sweetie.
Testing FSH: The Menopause Detective Work

Measuring FSH levels is a significant step in diagnosing menopause. It helps you get the inside scoop on your reproductive health.
The FSH test is typically done during the early follicular phase of your menstrual cycle – usually on day two or three after your period starts its monthly appearance.
This timing is crucial because FSH levels bounce around throughout your cycle like a caffeinated rabbit. Testing at this specific point gives doctors the clearest picture of what your ovaries are up to.
FSH Numbers Decoded:
FSH is measured in IU/L (International Units per Liter) or mIU/mL (milli-International Units per milliliter). Because medical science loves making things sound complicated.
Reproductive Years: FSH levels: 4.7 to 21.5 IU/L (or mIU/mL)
During Menopause: FSH levels begin to rise, often exceeding 30 IU/L
Post Menopause: FSH levels: 25.8 to 134.8 IU/L
Important note, darling: Normal ranges can vary between laboratories. They’re like recipes for chocolate cake – they vary between grandmas. Always check your specific lab’s range on your blood test report.
Interpreting FSH results can be trickier than parallel parking in stilettos. Individual variations, your age, and your overall health can all influence these hormone levels. That’s why it’s absolutely essential to sit down with your healthcare provider. Have a proper chat about what your FSH results mean for YOUR specific situation.
Beyond FSH testing, your doctor might also check your estrogen and LH levels. This helps them get the full picture of your hormonal status. It’s like assembling a puzzle, you need all the pieces to see the complete image.
Together, these tests help create a clearer picture of the changes happening in your fabulous body. They guide appropriate strategies for managing any symptoms that are cramping your style.
LH: The Prima Ballerina with Perfect Timing
If FSH is the stage manager, then LH is the prima ballerina. She delivers that show-stopping performance that makes the audience gasp. LH sweeps in mid-cycle with a dramatic surge to trigger ovulation. All while maintaining essential supporting roles throughout the entire hormonal ballet.

What’s the Deal with LH?
Luteinizing hormone (LH, because we’re all about efficiency here) is produced by your trusty pituitary gland. It works alongside FSH like a well-rehearsed dance partnership.
Together, they regulate ovarian function and keep your reproductive processes running smoother than a freshly waxed floor.
LH gets its name from “luteinize,” which means to form a corpus luteum. Now, before your eyes glaze over, darling, let me explain: the corpus luteum is this really important structure that forms after an egg is released from your ovary.
It’s basically a progesterone factory, pumping out the hormone needed to maintain early pregnancy. Nature’s pretty clever when she wants to be!
LH’s Starring Role in Reproduction
Picture this: mid-cycle, there’s a surge of LH that’s more dramatic than any soap opera plot twist. This surge triggers ovulation, the grand release of a mature egg from your ovary.
Once that egg makes its exit, the ruptured follicle transforms into the corpus luteum (remember that little factory?). It starts cranking out progesterone to thicken your uterine lining, preparing it for a potential pregnancy.
 LH also moonlights as a production assistant. It stimulates the creation of estrogen and progesterone in your ovaries. It’s all about maintaining that delicate hormonal balance necessary for reproduction. Think of it as a hormonal tightrope walk.
LH also moonlights as a production assistant. It stimulates the creation of estrogen and progesterone in your ovaries. It’s all about maintaining that delicate hormonal balance necessary for reproduction. Think of it as a hormonal tightrope walk.
If fertilization doesn’t happen (and let’s face it, most months it doesn’t), the corpus luteum breaks down like a temporary stage set.
Progesterone levels drop, and boom, menstruation begins. Cue the tampons and chocolate cravings!
When LH Levels Go Haywire During Menopause
During your reproductive years, LH levels follow a predictable pattern. They rise sharply mid-cycle to trigger ovulation like clockwork.
But as we age (or as I prefer to say, as we ripen into our full magnificence), the number of ovarian follicles naturally declines. This leads to decreased estrogen production by the ovaries.
 Your pituitary gland, sensing these lower estrogen levels like a smoke detector sensing trouble, responds by cranking up production of both LH and FSH.
Your pituitary gland, sensing these lower estrogen levels like a smoke detector sensing trouble, responds by cranking up production of both LH and FSH.
The result? Consistently high levels of both hormones. They’re like they’re permanently stuck on the “emergency” setting.
Over time, this persistent high level causes something called desensitization of the follicle receptors. Basically, the follicles become immune to these hormonal signals.
They’re like teenagers becoming immune to their parents’ nagging. They become less responsive, leading to irregular ovulation. This eventually stops altogether as menopause approaches. It’s the final curtain call for your reproductive years.
The Effects of LH’s Mood Swings
The fluctuation and eventual rise in LH and FSH levels contribute massively to the hormonal imbalance we associate with menopause.
While many symptoms are primarily linked to declining estrogen (she’s the real troublemaker), high and erratic LH levels, combined with fluctuating FSH, lead to irregular periods. The hormonal balance required for a regular menstrual cycle gets thoroughly disrupted.
However, darling, it’s crucial to note that everyone’s experience is different. Some women barely notice these changes. Others feel like they’re on a hormonal rollercoaster designed by someone with a twisted sense of humor. This reflects the wonderfully complex interplay between menopause hormones.
Testing LH: Another Piece of the Puzzle
LH plays a central role in women’s reproductive health. It goes through significant fluctuations during the menopausal transition. A simple blood test can measure LH levels. It’s often done alongside other tests to assess your reproductive health and menopausal status.
As women transition through menopause, LH levels change more dramatically than a reality TV personality’s career:

Pre-menopause: LH levels: 5 to 25 IU/L.
Postmenopause: LH levels: 14.2 to 52.3 IU/L.
For women in their 40s and 50s experiencing symptoms like irregular periods or hot flashes (welcome to the club, by the way), elevated LH levels in a blood test can indicate that menopause is approaching. It’s like a train you can’t stop.
However – and this is important, honey – LH testing isn’t done in isolation, like a solo performance. To get the complete picture of your hormonal status and confirm menopause, doctors typically consider multiple factors:
- LH levels
- FSH levels
- Estrogen levels
- Overall health
- Reported symptoms
This holistic approach allows healthcare providers to accurately assess where you are on your menopausal journey. They can then provide appropriate care and guidance. It’s like being a detective, but instead of solving crimes, you’re solving the mystery of your changing body!
Inhinin-B: The Quiet Supporting Dancer
 While the other hormones are taking center stage, Inhibin-B plays a crucial supporting role in this hormonal dance. She helps regulate FSH production from behind the scenes. She’s not flashy, but honey, she’s essential.
While the other hormones are taking center stage, Inhibin-B plays a crucial supporting role in this hormonal dance. She helps regulate FSH production from behind the scenes. She’s not flashy, but honey, she’s essential.
What Exactly Is Inhibin-B?
Inhibin-B is a hormone produced by your ovaries. Specifically, it comes from those small, growing follicles that contain immature eggs. Think of it as the backstage coordinator making sure FSH doesn’t get too big for its britches.
It plays a critical role in regulating FSH production. It does this by providing feedback to the pituitary gland in your brain.
Inhibin-B is part of the complex network of hormones managing your menstrual cycle. It offers valuable insights into how well your ovaries are functioning.
Inhibin-B’s Role in Baby-Making
Inhibin-B’s primary job is to keep FSH in check. During the early part of your menstrual cycle (the follicular phase, for those keeping score), rising FSH levels stimulate the growth of ovarian follicles.
As these follicles grow like little ambitious sprouts, they produce increasing amounts of Inhibin-B.
This Inhibin-B then taps the pituitary gland on the shoulder. It says, “Hey, ease up on the FSH production, would you?” This feedback loop ensures that only the strongest follicles continue to develop. Eventually, this leads to the selection of one dominant follicle that will release an egg during ovulation.

Therefore, Inhibin-B plays a key role in egg maturation and ovulation timing. It helps maintain a healthy and regular menstrual cycle. It’s like quality control for your reproductive system!
Inhibin-B Levels During Menopause
As we age and approach menopause (that inevitable destination we’re all heading toward), the number of ovarian follicles decreases. They decrease like guests leaving a party. This leads to lower production of Inhibin-B.
This decline typically begins during perimenopause, those fun years leading up to menopause when your body can’t decide if it’s coming or going.
With fewer follicles, there’s less Inhibin-B available to regulate FSH levels. As a result, FSH rises in a desperate attempt to stimulate the remaining follicles.
During menopause itself, defined as 12 consecutive months without a period (mark it on your calendar, darling!), Inhibin-B levels become very low or completely undetectable.
This is because the ovarian follicles are nearly depleted. They’re like a wine cellar after a particularly good party. There’s little to no Inhibin-B being produced.
The drop in Inhibin-B is a major marker of the transition into menopause. It illustrates the dramatic changes in ovarian function and hormone levels occurring during this time. It’s like watching your fertility take its final bow.
Effects of Changing Inhibin-B Levels
As Inhibin-B levels decline, it triggers an increase in FSH. They’re inversely related, like a seesaw. This decline also affects the quality and quantity of remaining ovarian follicles, impacting fertility.

For women in their late 30s and 40s, lower levels of Inhibin-B can serve as an early warning indicator. It signals reduced ovarian reserve, indicating that perimenopause and eventual menopause are approaching on the horizon.
However, and this is important, sweetie, low Inhibin-B levels alone, especially in younger women, are not definitive predictors of imminent menopause. Your body isn’t that straightforward (when is it ever?).
While Inhibin-B itself doesn’t directly cause symptoms, its changing levels reflect the underlying shifts in ovarian function and hormone imbalance. It’s like a canary in a coal mine, but for your ovaries.
Testing Inhibin B: Another Tool in the Diagnostic Toolbox
A blood test can determine Inhibin-B levels. Higher levels indicate a greater number of viable follicles and a lower likelihood of entering menopause soon. It’s like checking your reproductive bank account balance.
In younger women, Inhibin-B levels are typically higher during the early follicular phase of the menstrual cycle. This reflects healthy ovarian function.
As women approach menopause, Inhibin-B levels decline. They decline like the sun setting on your reproductive years. By menopause, Inhibin-B levels are often undetectable, the account is officially closed.
Although Inhibin-B alone isn’t used to diagnose menopause (it’s a supporting player, remember?), it can be a useful part of a comprehensive hormonal assessment. It helps doctors understand the status of your ovarian function in relation to other markers like FSH and estrogen.
This makes Inhibin-B a valuable component in the study of menopause hormones. It offers insights into the timing and progression of the menopausal transition. It’s another puzzle piece in understanding your unique journey.

Estrogen – (E2): The Star of the Show
 If hormones were a Broadway production, estrogen would be the principal dancer. She’s the one whose name is in lights, who gets the standing ovations, and who absolutely runs the show. Estrogen leads the female reproductive system with the grace and precision of a prima ballerina guiding an entire ballet performance.
If hormones were a Broadway production, estrogen would be the principal dancer. She’s the one whose name is in lights, who gets the standing ovations, and who absolutely runs the show. Estrogen leads the female reproductive system with the grace and precision of a prima ballerina guiding an entire ballet performance.
What’s Estrogen All About?
Estrogen is THE key hormone that plays a vital role in the female reproductive system. It’s one of the primary hormones regulating various functions throughout your body. Particularly in us fabulous females.
Produced mainly by your ovaries (with some help from fat tissue and the adrenal glands), estrogen is responsible for developing those lovely female secondary sexual characteristics. Breast development, regulating your menstrual cycle, and maintaining pregnancy. Basically, estrogen is what makes us women, well, womanly!
But honey, this hormone isn’t just about reproduction. Estrogen is also essential for bone health, cardiovascular function, and skin health. It’s like the ultimate multitasker, the hormone equivalent of a woman juggling career, family, and a social life while still looking fabulous.
There are actually three main types of estrogen, like a girl group with different members:
Estradiol – the Beyoncé of the group, the most common and potent form in premenopausal women
Estriol – primarily produced during pregnancy, like a temporary band member
Estrone – becomes the lead singer after menopause, taking over when estradiol retires
Estrogen’s importance makes it a significant focus when discussing hormones and menopause. Its levels change considerably during this transition, affecting various bodily functions like a domino effect in designer heels.
Estrogen’s Starring Role in Reproduction

Estrogen’s role in reproduction is more multifaceted than a diamond, darling. It acts at different stages throughout a woman’s reproductive life, always adapting to the current scene.
During your menstrual cycle, estrogen levels fluctuate. They fluctuate like your mood when you’re hangry, regulating the growth and release of eggs and preparing your body for potential pregnancy.
In the first half of the cycle (the follicular phase, for the technically inclined), rising estrogen levels help stimulate the growth of your uterine lining (endometrium).
This creates a plush, nourishing environment for a fertilized egg. Think of it as interior decorating for potential pregnancy.
As estrogen levels increase, they send signals to your brain. These signals reduce FSH production and increase LH. This hormonal shift triggers ovulation, where a mature egg is released from your ovary.
It’s like a debutante making her entrance at a ball. After ovulation, estrogen levels decline slightly. However, they’re still necessary to maintain that beautifully decorated uterine lining.
Estrogen also plays a crucial role in maintaining vaginal health. It ensures lubrication and elasticity, both important for sexual function and comfort.
Its influence extends to the overall health of your reproductive organs. This makes it an absolute cornerstone in discussions about hormones and menopause. When estrogen declines during menopause, the effects ripple throughout your entire body.
Estrogen Levels During Menopause: The Great Decline
During menopause, estrogen levels undergo a major decline. It would make the fall of Rome look subtle. This decline leads to many of the common symptoms associated with this transition. The ones we all know and some of us love to complain about over wine.
In the years leading up to menopause perimenopause, that delightful preview of what’s to come), estrogen levels fluctuate more wildly than stock market prices. These hormonal fluctuations are a hallmark of perimenopause. They can vary greatly from one woman to another. Some women experience dramatic swings. Others have a gentler transition. It’s all about your body’s unique personality.
As menopause progresses, your ovaries gradually produce less estrogen. This isn’t a sudden cliff drop (thank goodness). Rather, it’s a gradual descent, like a very slow elevator ride to a new floor of life. Eventually, this results in consistently low estrogen levels once you reach full menopause.
By the time menopause is confirmed, after 12 consecutive months without a menstrual period (mark that anniversary, darling!), estrogen levels have dropped significantly. This marks the end of your ovaries’ role as the primary producers of this hormone. They’re retiring, and honestly, after decades of service, can you blame them?
The reduction in estrogen during menopause affects multiple systems in your body. It’s like a ripple effect in a pond. Since estrogen helps maintain the health of reproductive tissues, bone density, and cardiovascular health, its decline is linked to common menopausal symptoms. These include hot flashes, night sweats, and an increased risk of osteoporosis.
Understanding these changes is essential in the broader conversation about hormones and menopause. Your body adjusts to a new hormonal balance. It’s like learning to dance to a completely different rhythm, it takes time and patience.
The Effects of Declining Estrogen: What You’re Actually Feeling
The decline in estrogen levels during menopause leads to a variety of symptoms. They’re collectively known as menopausal symptoms (as if you needed a fancy name for them!).

Hot flashes: Estrogen plays a substantial role in your body’s ability to regulate temperature. Therefore, its decline can cause your body to react with sudden heat. It’s like your internal thermostat has gone rogue and is being controlled by a mischievous gremlin.
Night sweats: These are hot flashes’ nocturnal cousins. They occur during sleep and often disrupt your rest, leading to fatigue. Because apparently, hot flashes during the day weren’t quite enough fun.
Mood swings and emotional changes: Estrogen levels impact neurotransmitter function in your brain. This influences mood and emotions. When estrogen fluctuates, so do your feelings. One minute you’re fine, the next you’re crying at a commercial featuring puppies.
Vaginal dryness: As estrogen levels decline, vaginal tissues may become less lubricated. Vaginal walls can thin. This can lead to discomfort and sexual dysfunction. These are direct effects of decreased estrogen affecting the health of vaginal tissues. Not exactly the sexy side of menopause, is it?
Bone density loss: Estrogen helps maintain bone strength. As a result, its reduction can lead to bone loss. This increases the risk of osteoporosis and fractures. Your bones quite literally need estrogen to stay strong and fabulous. Just like you need coffee to function in the morning.
Testing Estrogen: Getting the Numbers
Measuring estrogen levels can provide important insights into your menopausal status and overall hormonal health. Knowledge is power, darling!
Blood tests are commonly used to measure estradiol levels. Estradiol is the most potent form of estrogen. It’s the one doing most of the heavy lifting during your reproductive years.
Estrogen Numbers Decoded:
Estrogen levels are measured in picograms per milliliter (pg/mL). Because apparently, regular measurements weren’t confusing enough.
Reproductive Years: Estradiol levels: 30 to 400 pg/mL (quite a range, reflecting where you are in your cycle)
Perimenopause: Estradiol levels: They swing from high to low like a hormonal pendulum. However, they’re generally declining as menopause approaches
Post Menopause: Estradiol levels: below 30 pg/mL – the party’s officially over
These tests are often used alongside measurements of FSH and LH levels to diagnose menopause. High levels of FSH and LH, coupled with low estrogen levels, are the telltale signs. They indicate that menopause has arrived like an uninvited but inevitable guest.
However, because estrogen levels can fluctuate more wildly than a toddler’s attention span during the perimenopausal phase, a single test might not provide a complete picture. Doctors typically look at your symptoms, medical history, and other hormone levels to confirm a diagnosis. It’s detective work, really – hormonal CSI.
By understanding estrogen’s role and how its levels change during menopause, you can better prepare for the physical and emotional shifts. These shifts occur during this natural part of aging. Knowledge is power, and power looks fabulous on you, darling!
Progesterone (P4): The Ultimate Dance Partner
 If estrogen is the leading lady commanding center stage, then progesterone is her trusty sidekick. She’s the one who makes sure the show actually runs smoothly. These two hormones work together like a perfectly choreographed pas de deux. They maintain your menstrual cycle and prepare your body for pregnancy. They’re basically the Thelma and Louise of your reproductive system, minus the cliff diving.
If estrogen is the leading lady commanding center stage, then progesterone is her trusty sidekick. She’s the one who makes sure the show actually runs smoothly. These two hormones work together like a perfectly choreographed pas de deux. They maintain your menstrual cycle and prepare your body for pregnancy. They’re basically the Thelma and Louise of your reproductive system, minus the cliff diving.
What’s Progesterone All About?
Progesterone is a vital hormone. It plays an integral role in your fabulous female reproductive system. It’s produced mainly in your ovaries following ovulation, with some help from your adrenal glands (they like to chip in when they can).
During pregnancy, the placenta also gets in on the progesterone production action. This hormone’s main gigs? Preparing your body for conception, maintaining a pregnancy if one happens, and regulating your menstrual cycle like a well-organized event planner.
Progesterone’s Role in Baby-Making
Progesterone is essential for reproductive health. It works alongside estrogen like the ultimate dynamic duo.
After an egg is released from your ovary during ovulation (cue the fanfare), the remaining follicle transforms into a structure called the corpus luteum. This clever little structure then secretes progesterone like it’s its job. Because, well, it is.

This hormone prepares your uterine lining (endometrium) to receive and nourish a fertilized egg. It’s essentially rolling out the red carpet for potential pregnancy.
If fertilization occurs, progesterone levels remain high to support early pregnancy. They also prevent further ovulation. Because honey, one pregnancy at a time is quite enough, thank you very much.
If fertilization doesn’t occur (which, let’s be honest, is most months), progesterone levels drop. They drop faster than your energy on a Monday morning.
This leads to the shedding of the uterine lining, which results in menstruation. Cue the tampons, heating pads, and chocolate cravings.
Progesterone also helps maintain a healthy pregnancy. It does this by preventing contractions of the uterus, which could lead to premature labor. It’s basically the pregnancy bouncer, keeping everything calm and controlled.
Its role in regulating the menstrual cycle and supporting pregnancy makes progesterone a key focus. This is especially true when examining hormones and menopause. When this hormone starts declining, things get interesting.
Progesterone Levels During Menopause: The Great Exit
As you approach menopause and ovulation becomes less frequent (your ovaries are slowly checking out of the hotel), progesterone production gradually decreases. It’s like watching someone slowly fade from a party. First they’re there, then they’re sort of there, then suddenly they’ve left entirely.
By the time you reach menopause, defined as 12 months without a menstrual period (mark that anniversary with champagne, darling!) – progesterone levels are very low or completely absent. Ovulation ceases entirely. Your ovaries have officially retired from egg production.
The lack of progesterone can contribute to an increased risk of endometrial hyperplasia (thickening of the uterine lining). This happens if it’s not balanced with estrogen. It’s like having one partner leave the dance floor. The remaining one doesn’t quite know what to do alone.
Effects of Changing Progesterone Levels
The decline in progesterone levels during menopause has several noticeable effects on your body. And honey, some of them aren’t exactly subtle.
Your periods might become as unpredictable as British weather. They can be heavier or lighter, with spotting when you least expect it. They might skip cycles entirely as progesterone levels fluctuate. It’s like your menstrual cycle forgot how to read a calendar.

Low progesterone levels can also contribute to mood swings and irritability. Here’s why: progesterone has a calming effect on your brain and nervous system (it’s basically nature’s chill pill). When it declines, you might feel more on edge than usual. Suddenly, small annoyances become major grievances. You’re wondering why everyone around you is being so particularly irritating today.
Its decline can also lead to sleep disturbances, such as insomnia. This makes it difficult to get restful sleep. Between night sweats and declining progesterone, your bed becomes less of a sanctuary. It becomes more of a nightly battleground.
Additionally, progesterone’s role in maintaining bone health means that declining levels can contribute to the risk of osteoporosis. This is especially true when combined with decreasing estrogen levels. Your bones need both these hormones to stay strong and fabulous. Just like you need both coffee and wine to maintain your sanity.
These symptoms highlight the importance of progesterone in the context of hormones and menopause. Its reduction impacts both your physical and emotional well-being. It’s not just about hot flashes, darling – the whole hormonal orchestra is changing its tune.
Testing Progesterone: Getting the Numbers
Measuring progesterone levels can provide insights into your ovulatory status and reproductive health. This is especially true during the menopausal transition. Knowledge is power, sweetie!
Normal Progesterone Levels:
Progesterone is measured in nanograms per milliliter (ng/mL). Because regular measurements weren’t complicated enough, apparently.
Reproductive Years: Fluctuates during your menstrual cycle: less than 1 ng/mL to 20 ng/mL (quite the range, depending on where you are in your cycle)
Post Menopause: May fall below .5 ng/mL – the party’s officially over
While progesterone levels aren’t commonly used alone to diagnose menopause (it’s a team player, not a solo act), they can be part of a broader hormonal assessment. Measuring progesterone alongside estrogen and FSH can help provide a clearer picture. It shows where you are in the menopausal transition.
A combination of low progesterone, low estrogen, and high FSH levels typically indicates that you’re in menopause. It’s like collecting all the pieces of a puzzle to see the complete picture of your hormonal status.
AMH: The Understudy
AMH is like the understudy in this hormonal ballet. She’s quietly waiting in the wings, watching the performance. She gives us valuable insights into how many shows your ovaries have left in them. It offers a glimpse into the future of your fertility. It lets you know when the final curtain might fall.
What is AMH?
Anti-Müllerian Hormone (AMH, because that mouthful needed an abbreviation) is a protein hormone. It’s produced by the cells of developing ovarian follicles. Specifically, it comes from those small, early-stage follicles that are just getting started on their journey.
Unlike some other reproductive hormones that fluctuate more than your mood during PMS, AMH levels remain relatively constant throughout your menstrual cycle. This makes it a pretty reliable marker. It’s like that friend who’s always consistently punctual.
AMH serves as a marker of ovarian reserve. This refers to the number of eggs you have available for fertilization. Think of it as checking your reproductive bank account balance. As a result, it’s often used as a measure of your reproductive potential. How much “fertility currency” do you have in the vault?
AMH’s Role in Baby-Making
AMH plays an essential role in the early development of ovarian follicles. Those small sacs within your ovaries contain immature eggs. They’re like little treasure chests waiting to be opened.
By regulating the growth and maturation of these follicles, AMH helps ensure that a manageable number of eggs mature each cycle. It’s like a bouncer at an exclusive club. It makes sure not everyone gets in at once. AMH effectively helps maintain the pool of available eggs. It prevents too many from maturing simultaneously. Because your body knows that quality beats quantity, darling.
AMH levels are highest in women during their late twenties. This is generally considered the peak of fertility. It’s your reproductive prime time, baby! As you age (or as I prefer to say, as you ripen into your full magnificence), the number of remaining follicles decreases. This leads to a decline in AMH levels.
This decline serves as a natural indicator of diminishing ovarian reserve. It provides valuable information for assessing your reproductive lifespan. It’s like watching the gas gauge in your car. You know how much fuel you have left for the journey.
AMH Levels During Menopause: The Vanishing Act
AMH levels are closely tied to your ovarian reserve. Therefore, they change noticeably as you approach menopause. In fact, AMH is often one of the first hormones to wave goodbye.

In the years leading up to menopause (perimenopause, that delightful preview period), AMH levels decline. They can eventually become undetectable. It’s like watching someone slowly disappear into the fog.
The decline in AMH is one of the earliest signs of approaching menopause. It can occur years before other hormonal changes become apparent. It’s the early warning system. The canary in the coal mine. The first domino to fall.
Because of this, AMH is a valuable marker in the study of hormones and menopause. It offers insights into your fertility status long before menopause actually begins. It’s like getting advance notice of a party. You have time to prepare!
The Effects of Changing AMH Levels
Here’s the thing, honey: AMH itself doesn’t directly cause menopausal symptoms. It’s not the villain in this story. Instead, its levels provide an indication of ovarian reserve. They show the broader hormonal changes occurring as you approach menopause.
Typical AMH Levels
| AGE | AMH levels |
|---|---|
| 20–25 years | 4.23 ng/mL |
| 26–30 years | 3.48 ng/mL |
| 31–35 years | 2.43 ng/mL |
| 36–40 years | 1.28 ng/mL |
| 40–44 years | 0.52 ng/mL |
| AGE | AMH levels |
|---|---|
| 20–25 years | 4.23 ng/mL |
| 26–30 years | 3.48 ng/mL |
| 31–35 years | 2.43 ng/mL |
| 36–40 years | 1.28 ng/mL |
| 40–44 years | 0.52 ng/mL |
Low AMH levels signal a reduced number of viable eggs. This is associated with the onset of menopausal symptoms. Other hormones, like estrogen and progesterone, also begin to fluctuate and decline. It’s all interconnected, darling. When one domino falls, others follow.
Testing AMH: Your Fertility Backstage Pass

Measuring AMH levels can indicate your reproductive health. It helps predict menopause timing. A simple blood test can determine AMH levels. It provides an estimate of your ovarian reserve. Essentially, how many eggs you have left in your basket.
In younger women, higher AMH levels suggest a healthy ovarian reserve. Meanwhile, lower levels can indicate a reduced reserve. They might signal potentially earlier onset of menopause. It’s like checking your retirement account. The numbers tell you where you stand.
In terms of specific measurements, AMH levels are considered low if they’re below 1.0 ng/mL. This indicates a decreased ovarian reserve. During the menopausal transition, AMH levels often fall below 0.1 ng/mL. Essentially, the vault is nearly empty.
While AMH alone isn’t typically used to diagnose menopause (it’s a supporting player, not the star), it’s a useful indicator. When combined with other hormonal tests, such as FSH and estrogen, it provides a comprehensive picture of your hormonal health.
By understanding AMH and its role in your body, you can gain insights into your fertility. You can understand the timing of menopause. This empowers you to make informed decisions about your reproductive health. Knowledge is power, and power looks absolutely fabulous on you!
Testosterone (TES): Your Inner Strength Coach

Testosterone is the driving force behind energy and vitality in your fabulous female body. Like a dynamic soloist who steals the show, it enhances strength and endurance. It plays a crucial role in your overall well-being. Who knew this “male hormone” was one of your secret weapons?
What’s Testosterone Doing in a Woman’s Body?
Testosterone is commonly known as a male hormone (the boys get all the credit, don’t they?). However, it’s also produced in smaller amounts in us women. It comes primarily from our ovaries and adrenal glands. Surprise! We’ve got testosterone too, just in more refined quantities.
Testosterone is a key hormone that contributes to overall hormonal balance. This makes it an important part of the discussion on hormones and menopause. It’s like the supporting actor who deserves more recognition than they get.
Testosterone’s Role in Reproduction and Beyond
In women, testosterone’s role goes beyond reproduction. It regulates various bodily functions. These include bone density and muscle mass. It’s basically your body’s personal trainer, keeping things strong and functional.

During your reproductive years, testosterone levels are naturally higher. They profoundly influence reproductive tissues. They contribute to your libido (sex drive). Yes, darling, testosterone is partly responsible for that spark in your bedroom. Or wherever you choose to get frisky!
This androgen also supports the production of other key hormones in your female endocrine system. It’s a team player. It helps other hormones do their jobs more effectively.
The presence of testosterone is vital for a well-functioning reproductive system. It complements the roles of estrogen and progesterone. It’s like the third member of a girl group. Understanding testosterone’s role helps paint a complete picture. It shows how hormones work together to support your health. This is especially true during the transition to menopause.
Testosterone Levels During Menopause: The Subtle Decline
As you approach menopause, your hormone levels fluctuate. They fluctuate like a hormonal rollercoaster. Testosterone levels generally decline. However, they decline more gently than estrogen and progesterone’s dramatic exit.
Normal Testosterone levels:
Testosterone is measured in nanograms per deciliter (ng/dL). More medical measurements to keep track of!
| Age (years) | Female (ng/dL) |
|---|---|
| 18 and older |
|
This decrease can start in the years leading up to menopause. Perimenopause – that delightful transitional phase we all love so much. The reduction in testosterone is less pronounced compared to estrogen and progesterone’s dramatic plunge. However, it still plays a significant role in the overall changes you experience during this time.
By menopause, testosterone levels are typically lower than in your earlier reproductive years. Despite these lower levels, some women may experience an increase in the relative impact of testosterone. This happens due to the more significant drop in estrogen. It’s like when everyone leaves a party except two people. Suddenly those two seem much more prominent.
This can lead to symptoms such as increased facial hair (hello, tweezers!). It can also cause changes in skin texture. These shifts highlight the nuanced role of testosterone in the context of hormones and menopause. It’s all about the balance, darling.
The Effects of Changing Testosterone Levels
Low testosterone levels can manifest in several ways. They go beyond just a decrease in libido and reduced muscle mass. Symptoms include:
Fatigue: That bone-deep tiredness. No amount of coffee seems to fix it.

Mood changes: Increased irritability or feelings of depression. Suddenly everyone’s getting on your nerves more than usual.
Body composition changes: The balance between testosterone and estrogen shifts during menopause. This can affect the distribution of body fat. It leads to changes in where your body stores fat. Your waistline might expand. Fat might migrate to places it never visited before.
Reduced muscle mass: Maintaining muscle becomes harder. It’s like your muscles are staging a slow-motion walkout.
These changes in testosterone and other hormones illustrate the interconnected nature of hormones and menopause. They show how they influence your body and overall well-being. It’s all connected, sweetie. Change one hormone, and the whole system feels it.
Testing Testosterone: Another Piece of the Puzzle
A blood test can measure testosterone levels as part of a broader hormonal evaluation. This is particularly important if you’re experiencing symptoms that may be related to hormonal imbalance. Symptoms like low libido or unexplained fatigue make you want to nap at inappropriate times (like during important meetings).
While testosterone isn’t the primary hormone used to diagnose menopause (that honor goes to FSH and estrogen), measuring it can provide valuable insights. It reveals your overall hormonal health. It’s like checking all the instruments in the orchestra. This helps you understand the complete symphony.
Understanding testosterone levels in conjunction with other hormones like estrogen, FSH, and LH helps provide a comprehensive picture. It shows the hormonal changes occurring during menopause. Because darling, you’re not just dealing with one hormone going rogue. It’s the whole ensemble changing its tune!
The Grand Finale: Bringing It All Together
So there you have it, sweetheart. The complete cast of characters in your hormonal ballet! From GnRH, the director calling all the shots, to FSH and LH, the dynamic duo trying desperately to keep the show running.
Then there’s estrogen, the star whose exit changes everything, and progesterone, the trusty sidekick. Don’t forget the supporting players like Inhibin-B, AMH, and testosterone. They all work together in this intricate dance.
Understanding menopause hormones isn’t just about memorizing hormone names and numbers. Though your doctor will appreciate it if you do. It’s about recognizing that your body is going through a massive transition.
Every symptom you’re experiencing, from hot flashes to mood swings to that mysterious weight gain around your middle, is connected to this complex hormonal choreography.
If you want to see how all of this fits into the wider transition, phases, stages, and timing, start with STRAW+10: The Menopause Roadmap. STRAW+10 is the framework that names these phases and stages. If you want the quick, clear explanation, read What is STRAW+10?
The beautiful truth? Knowledge is power, darling. The more you understand about what’s happening in your fabulous body, the better equipped you are to navigate this journey. You can do it with grace, humor, and maybe a really good fan.
You’re not going crazy. You’re not falling apart. And you’re certainly not alone. You’re simply experiencing the natural evolution from one magnificent life stage to another.
So raise a glass (of water, wine, or whatever suits your fancy) to your hormones. They’ve served you well for decades. Even as they take their final bow, they’re still worth celebrating. After all, menopause isn’t the end of your story, darling. It’s just the beginning of your most powerful, unapologetic chapter yet.
Welcome to the club, you magnificent menopausal marvel. Now go forth and conquer. You’re armed with knowledge, humor, and the understanding that every hot flash is just your inner fire refusing to be dimmed! 🔥✨
Bisous et Bouffées de Chaleur (Kisses and Hot Flashes),
Your Partner in Hormonal Crime.




Leave a Comment